Avoiding atropine in glaucoma patients
Avoiding atropine in glaucoma patients is a rule. When treating patients with glaucoma, careful consideration must be given to any eye drops prescribed. One important rule is to avoid atropine or any strong dilating agents (mydriatics) in these patients.
Atropine is a muscarinic antagonist that works by blocking the parasympathetic stimulation of the eye. This leads to:
- Pupil dilation (mydriasis)
- Relaxation of the ciliary muscle
- Paralysis of accommodation (cycloplegia)
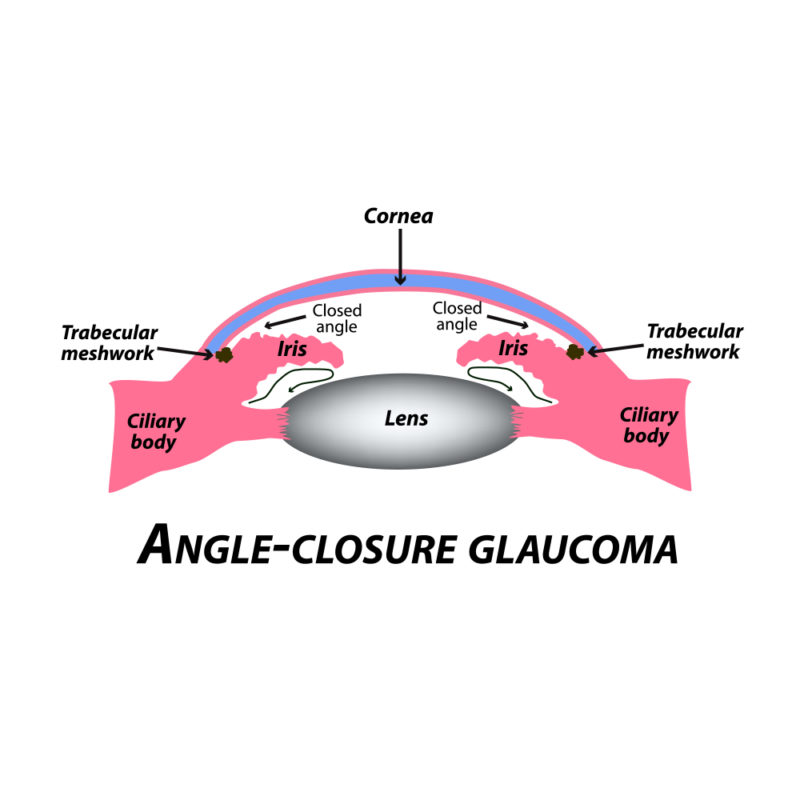
In patients with glaucoma, especially those with narrow or closed angles, these effects can be dangerous:
- Blocked Aqueous Humor Outflow
- Atropine dilates the pupil, and the iris moves closer to the trabecular meshwork.
- This can block the drainage angle and trap aqueous humor inside the eye.
- Sudden Rise in Intraocular Pressure (IOP)
- With outflow obstructed, intraocular pressure can shoot up rapidly, causing pain and vision loss.
- Triggering Acute Angle-Closure Glaucoma Attack
- In susceptible patients, even a single dose of atropine can precipitate a sight-threatening emergency.
Anti-glaucoma medications (like pilocarpine, beta blockers, prostaglandin analogs, etc.) are prescribed to lower IOP either by increasing aqueous outflow or reducing its production. Giving atropine alongside would reverse their effect and worsen the disease.
Atropine must be avoided in patients on anti-glaucoma treatment because it dilates the pupil, narrows the drainage angle, and can precipitate an acute rise in eye pressure-potentially leading to irreversible optic nerve damage.
In patients with glaucoma (especially on anti-glaucoma drugs), we avoid atropine and strong mydriatics. But sometimes we still need dilation:
Tropicamide (0.5–1%)
- Short-acting mydriatic (wears off in 4–6 hours).
- Causes pupil dilation with minimal effect on the anterior chamber angle, so it’s considered relatively safe.
- Preferred for fundus examination in glaucoma patients.
Phenylephrine (2.5%)
- A sympathomimetic that dilates the pupil by stimulating the dilator muscle.
- Does not paralyze accommodation (no cycloplegia).
- Usually used in combination with tropicamide for better dilation.
Founder of EyesMatterMost- an optometry student who loves talking about eyes. I tend to cover topics related to optometry, ophthalmology, eye health, eyecare, eye cosmetics and everything in between. This website is a medium to educate my readers everything related to eyes.